Efficacy: DMF Pivotal Trials
VUMERITY offers the efficacy demonstrated by dimethyl fumarate across 2 pivotal trials1
The efficacy of VUMERITY is based upon bioavailability studies in patients with relapsing forms of multiple sclerosis and healthy subjects comparing oral dimethyl fumarate (DMF) delayed-release capsules to VUMERITY delayed-release capsules. The clinical studies described below were conducted using dimethyl fumarate
2-year, randomized, double-blind, placebo-controlled trials in RRMS


Primary endpoint
Proportion of patients relapsed (PPR) at 2 years
Additional endpoints
The number of new or newly enlarging T2 hyperintense lesions, new T1 hypointense lesions, and gadolinium-enhancing (Gd+) lesions
ARR (annualized relapse rate)
Time to confirmed disability progression


Primary endpoint
ARR at 2 years
Additional endpoints
The number of new or newly enlarging T2 hyperintense lesions, new T1 hypointense lesions, and Gd+ lesions
PPR
Time to confirmed disability progression
Inclusion criteria in Study 1 and Study 2
Patients who had experienced at least 1 relapse over the year preceding the trial or had a brain magnetic resonance imaging (MRI) scan demonstrating at least 1 Gd+ lesion within 6 weeks of randomization
Patients' scores on the Expanded Disability Status Scale (EDSS) were assessed, and scores could range from 0 to 5
Exclusion criteria in Study 1 and Study 2
Patients who were treated with interferon-beta or glatiramer acetate within 3 months of randomization
Patients who had an infusion disease-modifying therapy or other selected therapies within 6 months of randomization
Patients with progressive forms of multiple sclerosis or any major disease that would preclude participation in a clinical trial
Evaluations in Study 1 and Study 2
Neurological evaluations were performed at baseline, every 3 months, and at the time of suspected relapse
MRI evaluations were performed at baseline, month 6, and years 1 and 2 in a subset of patients (44% in Study 1 and 48% in Study 2)
aThe starting dose for DMF was 120 mg BID or TID for the first 7 days, followed by an increase to 240 mg BID or TID.
bThe only approved and recommended dose for DMF is 240 mg BID.2
>70% of Treated Patients Were Relapse-free at 2 Years1,c,d
Percentage of patients who remained relapse-free at 2 years
Primary endpoint
Study 1
DMF
73%
vs
Placebo
54%
PPR was 27% vs 46% (P<0.0001)
49%
relative risk reduction
Study 2
DMF
71%
vs
Placebo
59%
PPR was 29% vs 41% (P=0.0020)
34%
relative risk reduction
Treated Patients Experienced <0.5 Relapse Every 2 Years, Based on ARR1
Annualized relapse rate over 2 years

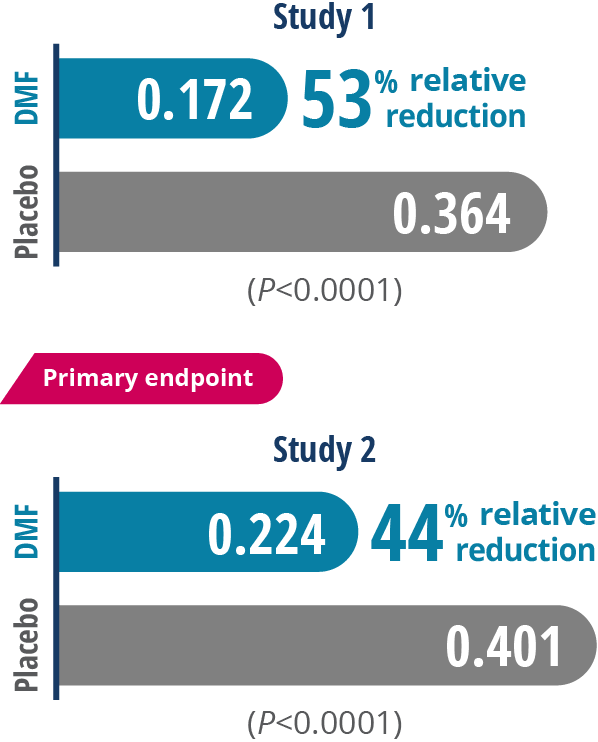
cRelapses were defined as new or recurrent neurologic symptoms not associated with fever or infection that lasted for at least 24 hours and were accompanied by new objective neurologic findings.
dThe percentage of relapse-free patients was calculated based on PPR at 2 years in Study 1 (100%–27%=73%) and Study 2 (100%–29%=71%).
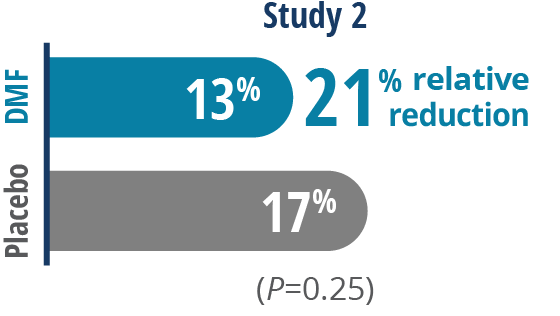
DMF May Reduce the Risk of Disability Progression1,e,f
Percentage of patients experiencing disability progression over 2 years
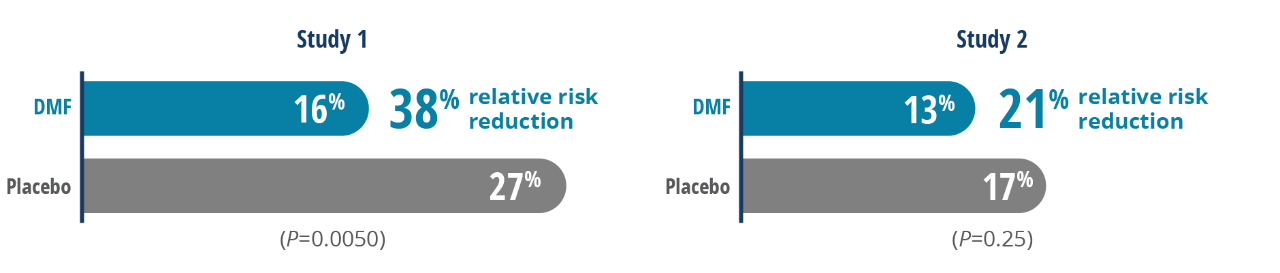
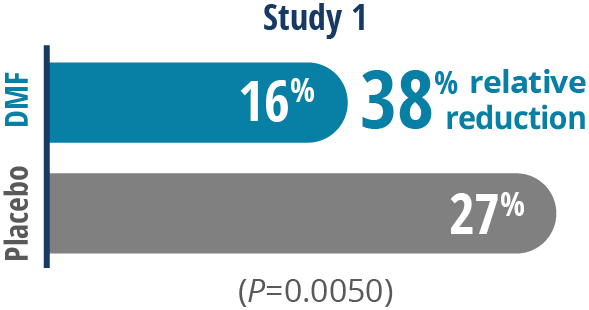
84%
of patients experienced NO DISABILITY PROGRESSION while taking dimethyl fumarate in Study 11
Not statistically significant
Most common adverse reactions (incidence for DMF [which has the same active metabolite as VUMERITY] ≥10% and ≥2% more than placebo) were flushing (40% vs 6%), abdominal pain (18% vs 10%), diarrhea (14% vs 11%), and nausea (12% vs 9%).1
eCalculated based on the percentage of patients experiencing disability progression in Study 1 (100%-16%=84%) and Study 2 (100%-13%=87%).1
fDisability progression was defined as at least a 1-point increase from baseline EDSS of ≥1, OR at least a 1.5-point increase for patients with baseline EDSS of 0 sustained for 12 weeks.
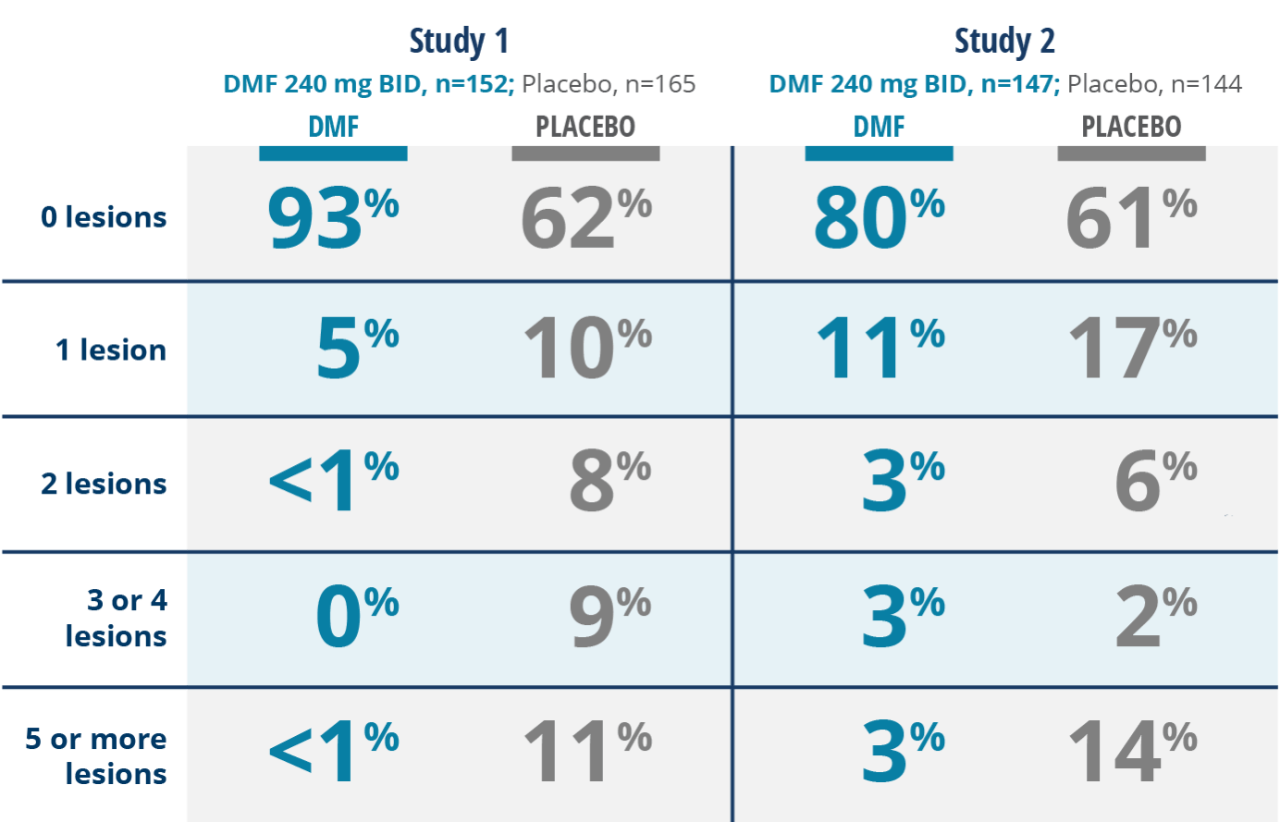
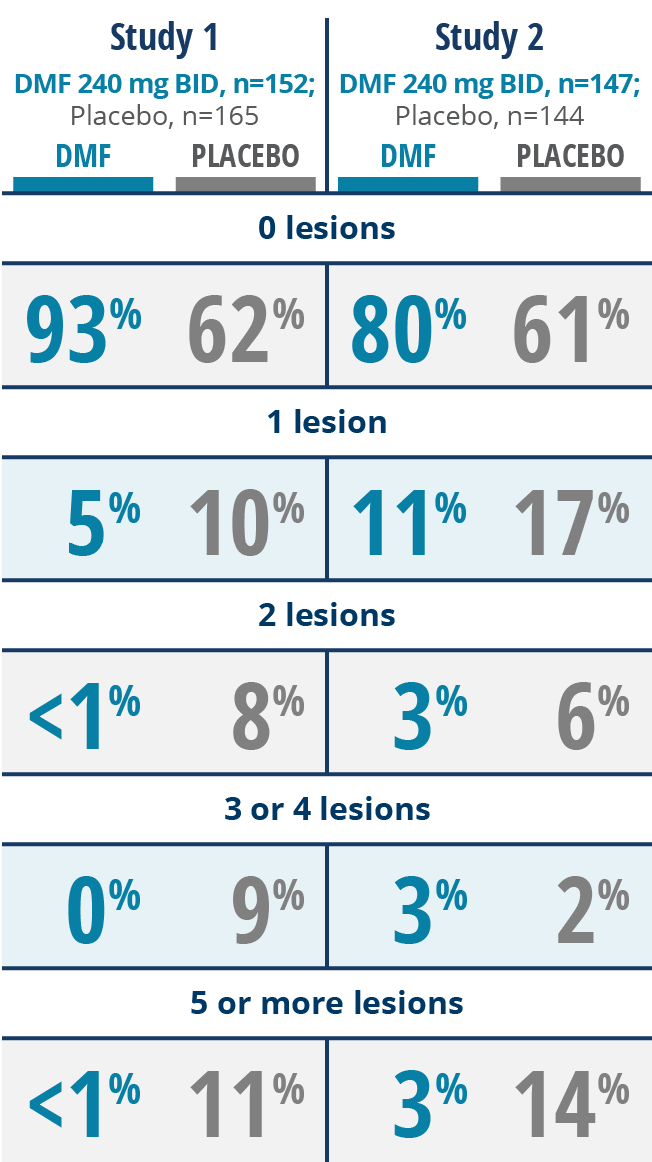
DMF Significantly Reduced Lesion Activity1,3-5
A relationship between MRI findings and clinical outcomes in RMS has not been established.
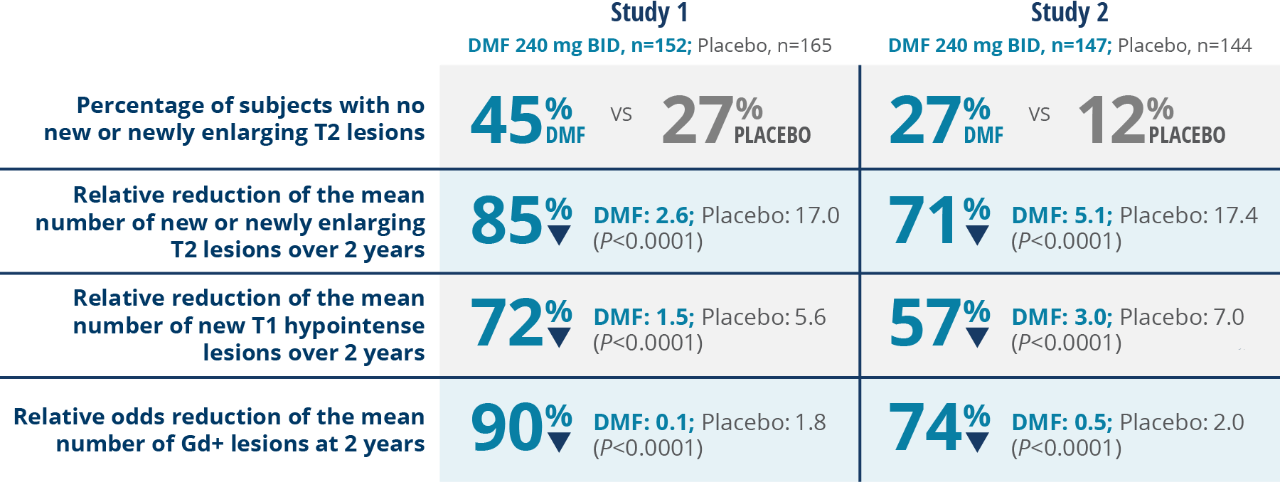
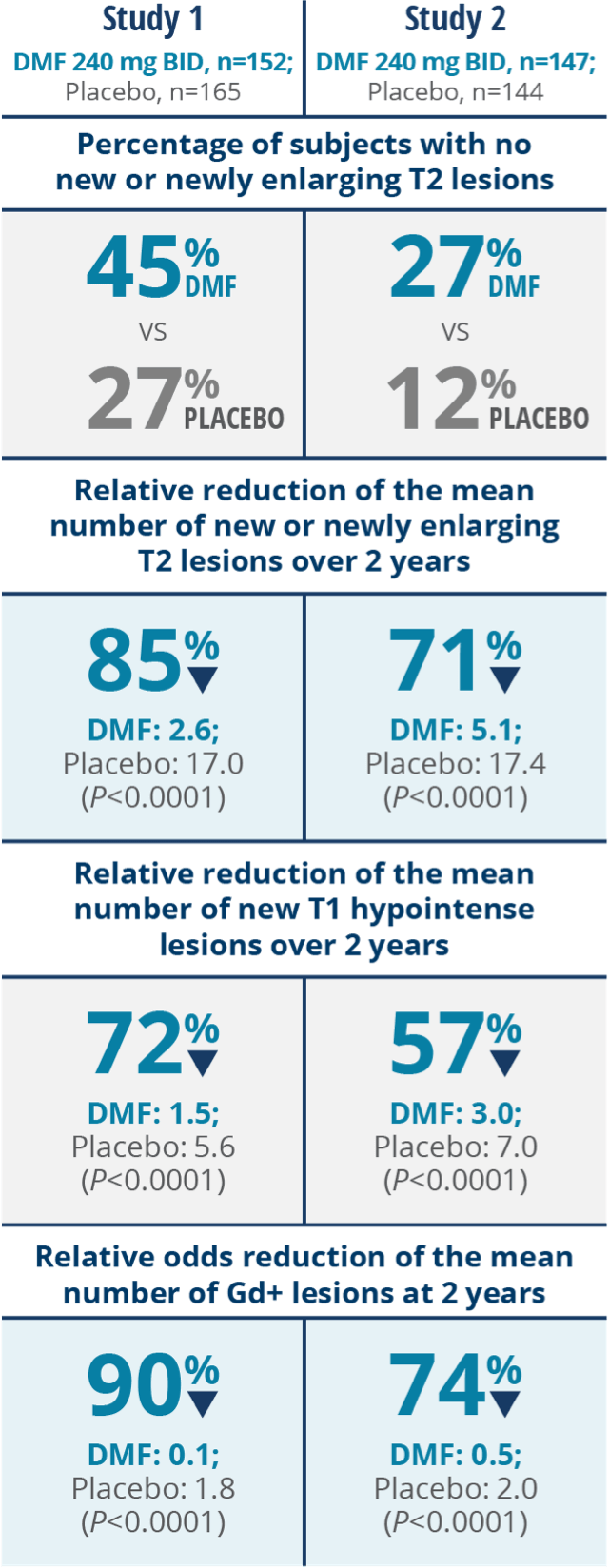
≥80% of Patients Taking Dimethyl Fumarate Had 0 Gd+ Lesions at 2 Years1
Percentage of subjects with Gd+ lesions at 2 years