Safety and Tolerability
VUMERITY offers the well-understood safety of dimethyl fumarate (DMF) with additional data on GI tolerability from patient-reported outcomes1,2
The data described in the following sections were obtained using dimethyl fumarate
delayed-release capsules, which have the same active metabolite as VUMERITY
delayed-release capsules, which have the same active metabolite as VUMERITY
Contraindications
VUMERITY is contraindicated in patients
- With known hypersensitivity to diroximel fumarate, dimethyl fumarate, or to any of the excipients of VUMERITY. Reactions may include anaphylaxis and angioedema
- Taking dimethyl fumarate
Warnings and Precautions
Anaphylaxis and Angioedema1
Warning
- Dimethyl fumarate can cause anaphylaxis and angioedema after the first dose or at any time during treatment
Signs and symptoms
- Include difficulty breathing, urticaria, and swelling of the throat and tongue
Guidance
- Patients should be instructed to discontinue VUMERITY and seek immediate medical care should they experience signs and symptoms of anaphylaxis and angioedema
Progressive Multifocal
Leukoencephalopathy (PML)1
Warning
- PML has occurred in patients with MS who have been treated with dimethyl fumarate
- PML is an opportunistic viral infection of the brain caused by the JC virus (JCV) that typically only occurs in patients who are immunocompromised, and that usually leads to death or severe disability
Details
- A fatal case of PML occurred in a patient who received dimethyl fumarate for 4 years while enrolled in a clinical trial
- The patient experienced prolonged lymphopenia (lymphocyte counts predominantly <0.5×109/L for 3.5 years) while taking dimethyl fumarate
- PML has also occurred in the postmarketing setting in the presence of lymphopenia (<0.9x109/L)
- While the role of lymphopenia in these cases is uncertain, the PML cases have occurred predominantly in patients with lymphocyte counts <0.8x109/L persisting for more than 6 months
Signs and symptoms
- Diverse, progress over days to weeks
- Include progressive weakness on one side of the body or clumsiness of limbs; disturbance of vision; and changes in thinking, memory, and orientation leading to confusion and personality changes
- MRI findings may be apparent before clinical signs or symptoms
Guidance
- At the first sign or symptom suggestive of PML, withhold VUMERITY and perform an appropriate diagnostic evaluation
For additional information, please see full Prescribing Information.
Herpes Zoster and Other Serious Opportunistic Infections
Warning
- Serious cases of herpes zoster have occurred with dimethyl fumarate (which has the same active metabolite as VUMERITY), including disseminated herpes zoster, herpes zoster ophthalmicus, herpes zoster meningoencephalitis, and herpes zoster meningomyelitis
- These events may occur at any time during treatment
- Other serious opportunistic infections have occurred with dimethyl fumarate, including cases of serious viral (herpes simplex virus, West Nile virus, cytomegalovirus), fungal (Candida and Aspergillus), and bacterial (Nocardia, Listeria monocytogenes, Mycobacterium tuberculosis) infections
- These infections have been reported in patients with reduced absolute lymphocyte count (ALC) as well as in patients with normal ALC
- These infections have affected the brain, meninges, spinal cord, gastrointestinal tract, lungs, skin, eye, and ear
Guidance
- Monitor patients for signs and symptoms of herpes zoster
- Patients with symptoms and signs consistent with any of the serious opportunistic infections should undergo prompt diagnostic evaluation and receive appropriate treatment
- Consider withholding VUMERITY treatment in patients with herpes zoster or other serious infections until the infection has resolved
Lymphopenia1
Warning
- VUMERITY may decrease lymphocyte counts
Details
- In the MS placebo-controlled trials with dimethyl fumarate, mean lymphocyte counts decreased by approximately 30% during the first year of treatment with dimethyl fumarate and then remained stable
- Four weeks after stopping dimethyl fumarate, mean lymphocyte counts increased but did not return to baseline
- 6% of dimethyl fumarate patients and <1% of placebo patients experienced lymphocyte counts <0.5x109/L (lower limit of normal 0.91x109/L)
- In controlled and uncontrolled clinical trials with dimethyl fumarate, 2% of patients experienced lymphocyte counts <0.5x109/L for at least six months, and in this group the majority of lymphocyte counts remained <0.5x109/L with continued therapy
- Neither VUMERITY nor dimethyl fumarate has been studied in patients with preexisting low lymphocyte counts
Guidance
- Obtain a CBC, including lymphocyte count, before initiating treatment with VUMERITY, 6 months after starting treatment, and then every 6 to 12 months thereafter, and as clinically indicated
- Consider interruption of VUMERITY in patients with lymphocyte counts <0.5x109/L persisting for more than 6 months
- Given the potential for delayed recovery of lymphocyte counts, continue to obtain lymphocyte counts until their recovery if VUMERITY is discontinued or interrupted due to lymphopenia
- Restart VUMERITY based on individual and clinical circumstances
Liver Injury1
Warning
- Clinically significant cases of liver injury have been reported in patients treated with dimethyl fumarate in the postmarketing setting
- The onset has ranged from a few days to several months after initiation of treatment with dimethyl fumarate
- None of the reported cases resulted in liver failure, liver transplant, or death. Some cases required hospitalization
- The combination of new serum aminotransferase elevations with increased levels of bilirubin caused by drug-induced hepatocellular injury is an important predictor of serious liver injury that may lead to acute liver failure, liver transplant, or death in some patients
Signs and symptoms
- Include elevation of serum aminotransferases to greater than 5-fold the ULN and elevation of total bilirubin to greater than 2-fold the ULN
Guidance
- Obtain serum aminotransferase, alkaline phosphatase, and total bilirubin levels prior to treatment with VUMERITY and during treatment, as clinically indicated
- Discontinue VUMERITY if clinically significant liver injury induced by VUMERITY is suspected
Flushing1
Warning
- VUMERITY may cause flushing. In clinical trials, 40% of patients treated with dimethyl fumarate experienced flushing
- 3% of patients discontinued dimethyl fumarate for flushing and <1% had serious flushing symptoms that were not life-threatening but led to hospitalization
Signs and symptoms
- Generally began soon after initiating dimethyl fumarate and usually improved or resolved over time
- Include warmth, redness, itching, and/or burning sensation
Guidance
- Taking VUMERITY with food may reduce the incidence of flushing
- Alternatively, taking non-enteric coated aspirin (up to a dose of 325 mg) 30 minutes prior to VUMERITY dosing may reduce the incidence or severity of flushing
- Advise patients to contact their healthcare provider if they experience persistent and/or severe flushing
Serious Gastrointestinal Reactions1
Warning
- Serious gastrointestinal reactions, including perforation, ulceration, hemorrhage, and obstruction, some with fatal outcomes, have been reported in the postmarketing setting with the use of fumaric acid esters, including VUMERITY, with or without concomitant aspirin use
Details
- The majority of these events have occurred within 6 months of fumaric acid ester treatment initiation
- In controlled clinical trials, the incidence of serious gastrointestinal adverse reactions was 1% in patients treated with dimethyl fumarate; these events, none of which were fatal, included vomiting (0.3%) and abdominal pain (0.3%)
Guidance
- Monitor patients, promptly evaluate, and discontinue VUMERITY for new or worsening severe gastrointestinal signs and symptoms
Pivotal trial study design1
The efficacy and safety of dimethyl fumarate were demonstrated in 2 studies (Study 1 and Study 2), both of which enrolled patients with RRMS who had experienced at least 1 relapse over the year preceding the trial or had an MRI scan demonstrating at least 1 gadolinium-enhancing lesion within 6 weeks prior to randomization.
Study 1: a 2-year, randomized, double-blind, placebo-controlled study in which 1234 patients with RRMS were randomized to receive dimethyl fumarate 240 mg BID (n=410), dimethyl fumarate 240 mg TID (n=416), or placebo (n=408).
Study 2: a 2-year, randomized, double-blind, placebo-controlled study in which 1417 patients with RRMS were randomized to receive dimethyl fumarate 240 mg BID (n=359), dimethyl fumarate 240 mg TID (n=345), an open-label comparator (n=350), or placebo (n=363).
The only approved dose of dimethyl fumarate is the 240 mg BID dose.
The adverse reactions presented in the table below are based on safety information from 769 patients treated with dimethyl fumarate 240 mg twice a day and 771 placebo-treated patients.
The most common adverse reactions (incidence ≥10% and ≥2% more than placebo) were flushing, abdominal pain, diarrhea, and nausea.
Adverse reactions in Study 1 and Study 2 reported for dimethyl fumarate
240 mg BID at ≥2% higher incidence than placebo
| DMF n=769 |
Placebo n=771 |
|
|---|---|---|
| Flushing | 40% | 6% |
| Abdominal pain | 18% | 10% |
| Diarrhea | 14% | 11% |
| Nausea | 12% | 9% |
| Vomiting | 9% | 5% |
| Pruritus | 8% | 4% |
| Rash | 8% | 3% |
| Albumin urine present | 6% | 4% |
| Erythema | 5% | 1% |
| Dyspepsia | 5% | 3% |
| Aspartate aminotransferase increased | 4% | 2% |
| Lymphopenia | 2% | <1% |
GI Events
- Dimethyl fumarate caused GI events (eg, nausea, vomiting, diarrhea, abdominal pain, and dyspepsia)
- 4% of patients treated with dimethyl fumarate and less than 1% of placebo patients discontinued due to GI events
- The incidence of serious GI events was 1% in patients treated with dimethyl fumarate
- The incidence of GI events was higher early in the course of treatment (primarily in month 1) and usually decreased over time in patients treated with dimethyl fumarate compared with placebo
- Serious gastrointestinal (GI) reactions, including perforation, ulceration, hemorrhage, and obstruction, some with fatal outcomes, have been reported in the postmarketing setting with the use of fumaric acid esters, including VUMERITY, with or without concomitant aspirin use
Hepatic Transaminases
- An increased incidence of elevations of hepatic transaminases in patients treated with dimethyl fumarate was seen primarily during the first 6 months of treatment, and most patients with elevations had levels <3 times the ULN during controlled trials
- Elevations of alanine aminotransferase and aspartate aminotransferase to ≥3 times the ULN occurred in a small number of patients treated with both dimethyl fumarate and placebo and were balanced between groups
- No elevations in transaminases ≥3 times the ULN with concomitant elevations in total bilirubin >2 times the ULN
- Discontinuations due to elevated hepatic transaminases were <1% and were similar in patients treated with dimethyl fumarate or placebo
Eosinophilia
- A transient increase in mean eosinophil counts was seen during the first 2 months of therapy
Study was funded by Biogen.
EVOLVE-MS-2 study design1
- EVOLVE-MS-2 was a phase 3, randomized, head-to-head, active-controlled, 5-week study to evaluate patient-assessed GI tolerability of VUMERITY versus dimethyl fumarate in patients with RRMS
- The EVOLVE-MS-2 study used an adaptive trial design in which data from Part A were used to evaluate the utility of GI symptom scales and to inform the GI tolerability endpoints and sample size for Part B
- Parts A and B were identical in study assessments. Following the completion of Part A, a planned, unblinded analysis of GI tolerability was performed to refine the primary endpoint to reflect the most sensitive measure for detecting a difference between VUMERITY and dimethyl fumarate and re-estimate sample size


Patients who completed EVOLVE-MS-2 could roll over into EVOLVE-MS-1, a 96-week open-label study
aIn study week 1, the titrated dose for VUMERITY was one 231-mg delayed-release capsule taken orally, twice daily. The titrated dose for dimethyl fumarate was one 120-mg delayed-release capsule taken orally, twice daily. From study weeks 2–5, the full dose for VUMERITY was two 231-mg delayed-release capsules taken orally, twice daily, and the full dose for dimethyl fumarate was one 240-mg delayed-release capsule taken orally, twice daily.
Limitations and disclosures
- The GI symptom intensity scales are not validated
- Results should be interpreted with caution due to the 5-week duration
- Patients were excluded if they had a history of GI surgery, clinically significant recurring or active GI symptoms within 3 months of screening, or chronic use of medical therapy to treat GI symptoms within 1 month of screening
- The results from this study are not included in the full Prescribing Information for VUMERITY. The US Food and Drug Administration did not consider the results of this study when approving VUMERITY
Key eligibility criteria
- Patients aged 18–65 years with a confirmed RRMS diagnosis
- Patients had no history of GI surgery, clinically significant recurring or active GI symptoms within 3 months of screening, or chronic use of medical therapy to treat GI symptoms within 1 month of screening
GI tolerability assessments
- Patients used 2 GI tolerability scales to self-assess the duration and severity of their GI symptoms (nausea, vomiting, upper abdominal pain, lower abdominal pain, and diarrhea) on an 11-point patient-reported numerical rating scale using eDiaries
- Individual Gastrointestinal Symptom and Impact Scale (IGISIS): patients self-assessed the intensity of each of the 5 GI symptoms twice daily, within 9 hours of taking each dose
- Global Gastrointestinal Symptom and Impact Scale (GGISIS): patients self-assessed the intensity of any GI symptoms over the last 24 hours
Primary endpoint
- Number of days (relative to exposure) with any individual GI symptom intensity score ≥2 in the overall population
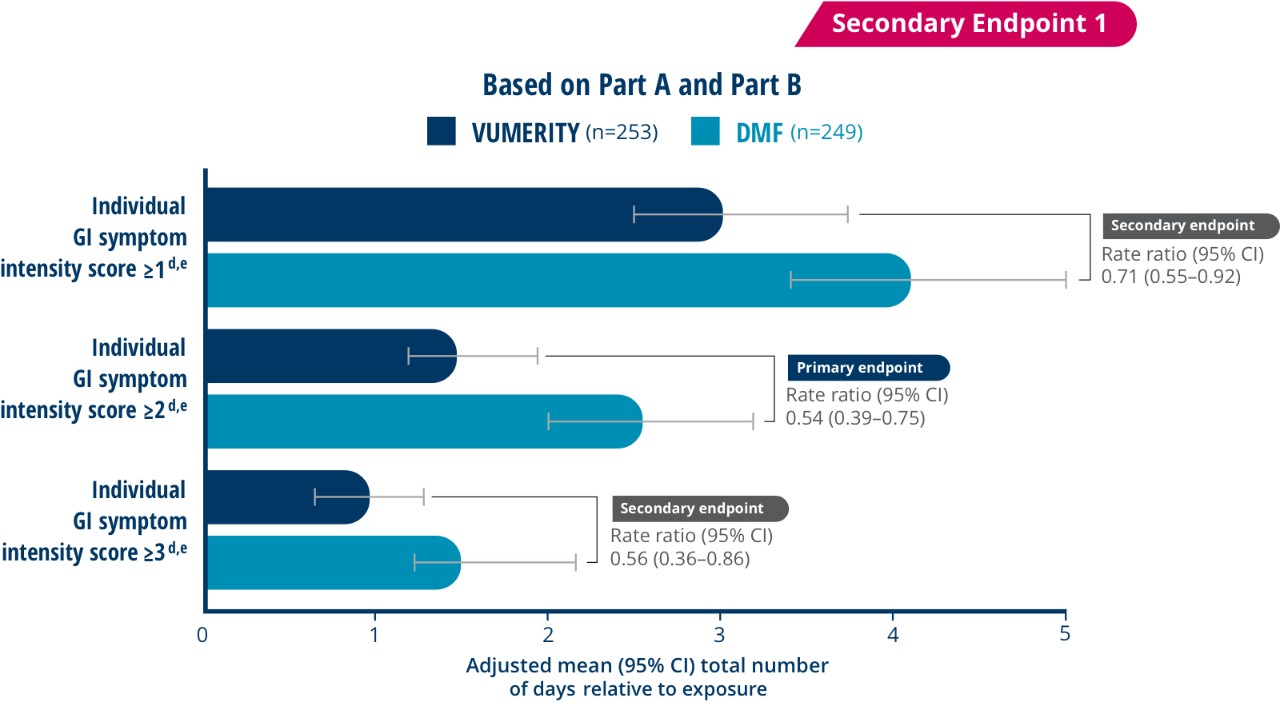
Secondary endpoints
- Number of days (relative to exposure) with individual GI symptom intensity scores of ≥1 or ≥3 in the overall population
- Number of days (relative to exposure) with an individual GI symptom intensity score of ≥2 in patients from Part B only
- Number of days (relative to exposure) with global GI symptom intensity scores of ≥1, ≥2, or ≥3 in the overall population
- Worst individual GI symptom score by study week
Patients self-reported 46% fewer days (relative to exposure) with GI symptoms on VUMERITY vs dimethyl fumarate
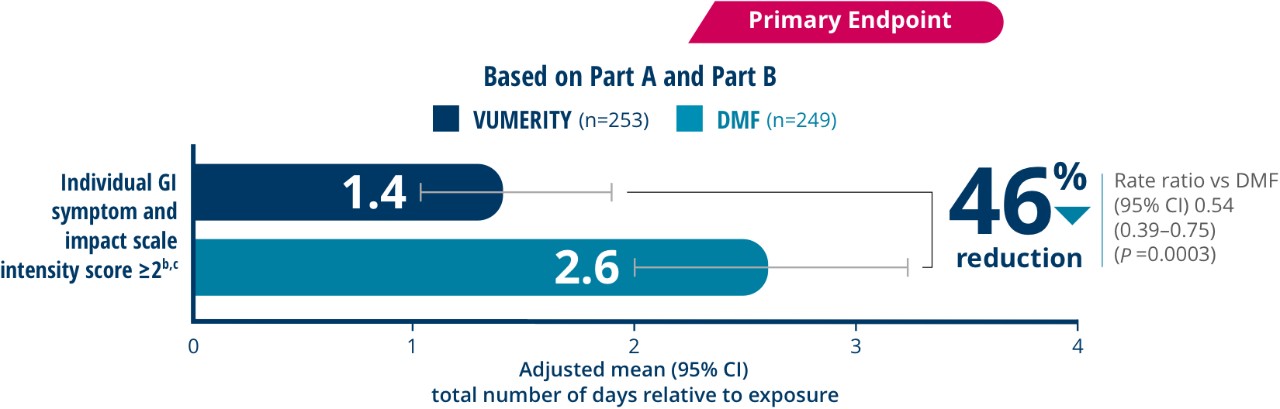

Over a 5-week treatment period, VUMERITY showed a 46% reduction (P=0.0003) in the number of days (adjusted rate ratio, 0.54 [95% CI, 0.39–0.75]) patients experienced a GI symptom rated ≥2 on a 0- to 10-point individual GI symptom and impact scale
Overall, 19.3% of patients (17 out of 88) in the VUMERITY group and 30.6% of patients (37 out of 121) in the DMF group used concomitant medications to treat GI-related AEs during the treatment period
- Days were not consecutive
- Patients taking VUMERITY reported fewer days with an individual GI symptom intensity score of ≥2 in an analysis of data collected from Part B only (adjusted rate ratio, 0.52 [95% Cl, 0.36-0.76])
bIntensity of nausea, vomiting, upper abdominal pain, lower abdominal pain, and diarrhea reported twice per day. cPatients completed ≥1 postbaseline tolerability eDiary assessment and were included in the analysis of patient-assessed GI tolerability.
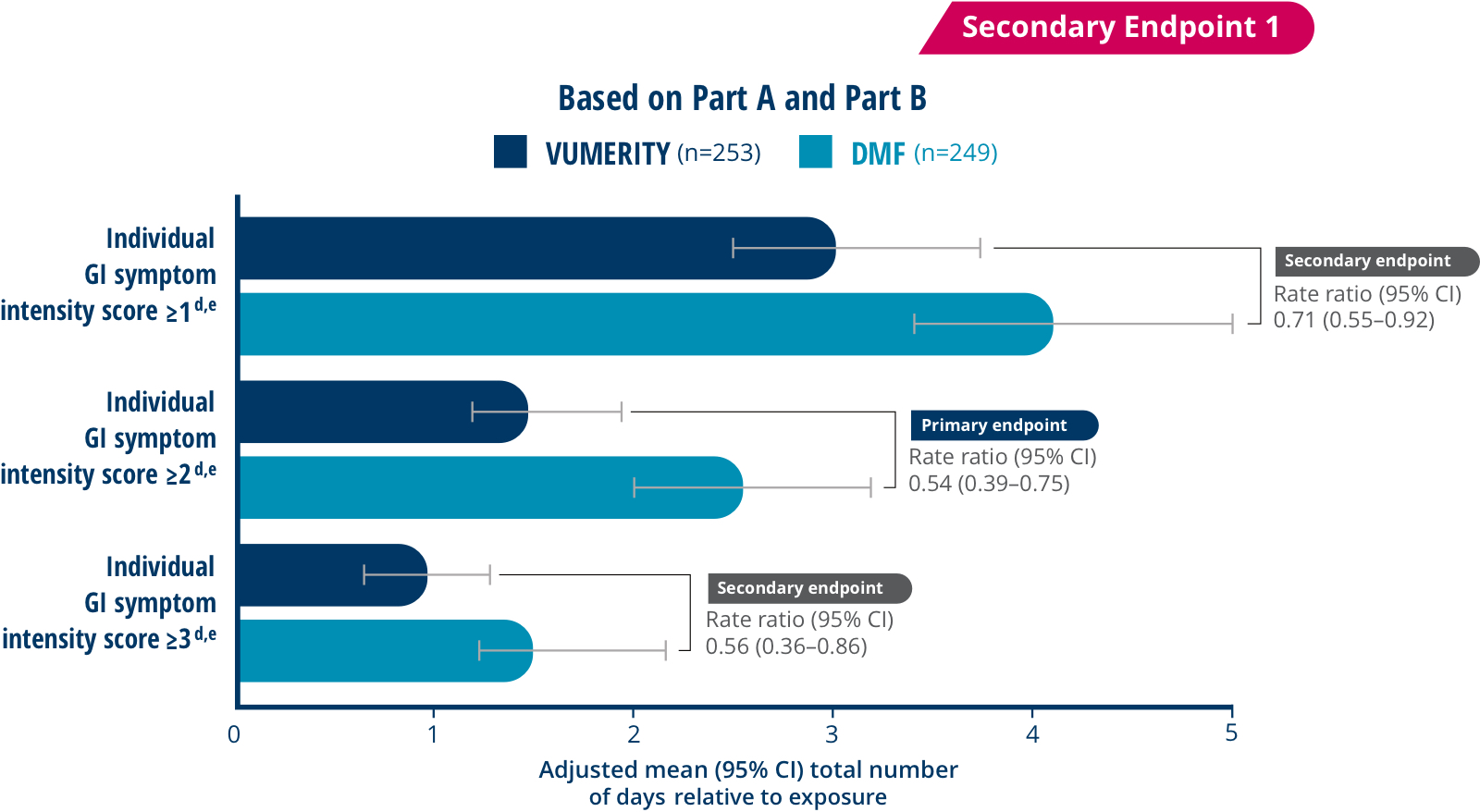
- Days were not consecutive
- Patients taking VUMERITY reported fewer days with an individual GI symptom intensity score of ≥2 in an analysis of data collected from Part B only (adjusted rate ratio, 0.52 [95% Cl, 0.36-0.76])
dIntensity of nausea, vomiting, upper abdominal pain, lower abdominal pain, and diarrhea occurring within the last 9 hours of taking the study drug. eCompleted ≥1 postbaseline tolerability eDiary assessment and were included in the analysis of patient-assessed GI tolerability.
VUMERITY patients reported fewer days with a global GI symptom intensity
score of ≥1, ≥2, or ≥3 compared to patients taking dimethyl fumarate2


- Days were not consecutive
- Patients taking VUMERITY reported fewer days with GI symptoms rated ≥1, ≥2, or ≥3 on the 0 to 10-point global GI symptom and intensity scale
- Upper GI events (upper abdominal pain, nausea, and vomiting) were less severe with VUMERITY. Lower GI symptoms (lower abdominal pain and diarrhea) were similar between VUMERITY and dimethyl fumarate
fIntensity of nausea, vomiting, upper abdominal pain, lower abdominal pain, and diarrhea occurring within the last 9 hours of taking the study drug. gCompleted ≥1 postbaseline tolerability eDiary assessment and were included in the analysis of patient-assessed GI tolerability.


hAnalysis of covariance model; factors include study parts, region (United States and non-United States), age, and body mass index.
<1% of patients discontinued VUMERITY due to GI AEs
Disposition of Patients With RRMS in EVOLVE-MS-2
| Patients, n (%) | VUMERITYi n=253 |
DMFi n=251 |
|---|---|---|
| Received ≥1 dose of study drug | 253 (99.6) | 251 (99.6) |
| Completed the treatment period | 245 (96.8) | 233 (92.8) |
| Mean (SD) days of treatment exposure, IGISISj | 35.2 (4.2) | 34.2 (5.9) |
| Mean (SD) days of treatment exposure, GGISISj | 33.3 (4.8) | 32.6 (5.6) |
| Rolled over to EVOLVE-MS-1 | 239 (94.5) | 225 (89.6) |
| Discontinued the study | 8 (3.2) | 18 (7.2) |
| AE leading to discontinuation during the treatment period | 4 (1.6) | 14 (5.6) |
| GI AE leading to discontinuation | 2 (0.8) | 12 (4.8) |
| Upper abdominal pain | 0 | 5 (2.0) |
| Diarrhea | 1 (0.4) | 3 (1.2) |
| Abdominal pain | 0 | 3 (1.2) |
| Vomiting | 1 (0.4) | 2 (0.8) |
| Abdominal distension | 0 | 1 (0.4) |
| GI pain | 0 | 1 (0.4) |
| Nausea | 0 | 1 (0.4) |
iPatients were randomized.
jVUMERITY, n=253; DMF, n=251.

fewer discontinuations due to GI adverse events compared to dimethyl fumarate (0.8% of patients taking VUMERITY vs 4.8% of patients taking DMF)
GI AEs Experienced in ≥5% of Patients in Either Group2
| System organ class preferred term, n (%) | VUMERITY n=253 |
DMF n=251 |
|---|---|---|
| Any AE | 198 (78.3) | 210 (83.7) |
| GI disorders | 88 (34.8) | 123 (49.0) |
| Diarrhea | 39 (15.4) | 56 (22.3) |
| Nausea | 37 (14.6) | 52 (20.7) |
| Upper abdominal pain | 17 (6.7) | 39 (15.5) |
| Abdominal pain | 16 (6.3) | 24 (9.6) |
| Lower abdominal pain | 15 (5.9) | 17 (6.8) |
| Vomiting | 9 (3.6) | 22 (8.8) |


Study was funded by Biogen.
Strategies to Help Your Patients Manage Common Side Effects1,3
Empower your patients from the start by setting expectations around flushing and GI symptoms
Most Common Adverse Events: Flushing and GI events. Please see adverse events above for additional information.
| Help Mitigate Flushing and GI Events | |
|---|---|
Flushing |
Over-the-Counter Options: Administration With Food:
|
GI Events |
Fox E, et al 2016 Study Design: Limitations: Over-the-Counter Options: |
| Dose Adjustment | |
|
Temporary dose reductions to 231 mg twice daily may help in managing tolerability for individuals who cannot tolerate the maintenance dose.
|
|
Nurse Educators can help
Nurse Educators can help patients understand what to expect while on treatment, help manage common side effects, and provide education about additional resources.
|
|